But there's a good chance what you're actually seeing is Rejection Sensitive Dysphoria.
RSD is not a personality quirk. It's not a trauma response. And it's not anxiety wearing a different coat. For clinicians and coaches working with ADHD adults, understanding the distinction changes everything — what you look for, how you respond, and what interventions actually help.
This guide equips ADHD coaches, therapists, and mental health providers with a working clinical understanding of RSD: what it is neurologically, how it presents in high-achieving adult clients, where misdiagnosis most commonly occurs, and how to actively support clients through it.
Key Takeaways
- RSD is an intense emotional response to perceived rejection, criticism, or failure — neurologically rooted in ADHD, not a character flaw
- It is not a DSM-5 diagnosis but leading ADHD clinicians treat it as a core feature of adult ADHD presentation
- In high-achieving adults, RSD fuels people-pleasing, perfectionism, and avoidance — often mistaken for professionalism
- Standard psychotherapy has limited reach during acute RSD episodes — a multi-modal toolkit is essential
- ADHD coaches are well-positioned to help clients build RSD-aware systems and insight between episodes
What Is Rejection Sensitive Dysphoria? A Clinical Overview
RSD is best understood as an extreme and sudden emotional response triggered by the perception of being rejected, criticized, teased, or having fallen short of a standard — whether that standard was set by others or by the person themselves.
The word "dysphoria" signals the clinical weight here. Derived from the Greek for "difficult to bear," it is not a descriptor of heightened sensitivity. It describes overwhelming emotional pain that arrives suddenly and feels impossible to reason through in real time.
Diagnostic Landscape
RSD does not appear as a standalone diagnosis in the DSM-5. As Dr. William Dodson — a leading ADHD clinician and one of the primary architects of the RSD framework — has noted, ADHD diagnostic criteria have never formally addressed emotional or mood-regulation problems, despite emotion dysregulation being one of the most functionally impairing aspects of the condition for many adults.
RSD is a real, recognized, and highly impairing phenomenon that sits outside the formal diagnostic taxonomy. Professionals should treat it as a clinically significant feature of adult ADHD — not an afterthought.
Key prevalence data worth knowing:
- A 2023 qualitative study found 33 of 43 young adults with ADHD reported RSD-like experiences
- Dodson's clinical observation places roughly one-third of adolescents and adults identifying RSD as the most impairing aspect of their ADHD
- Population-level prevalence data remains a significant evidence gap
Two Primary Presentations
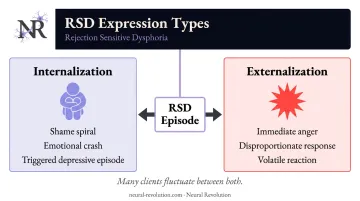
Professionals will typically observe RSD expressed in one of two ways — and many clients fluctuate between both depending on context:
- Internalization: Sudden emotional crash, shame spiral, or what appears to be a triggered depressive episode. Dodson describes this as looking like "an instantaneous but triggered major depression."
- Externalization: Immediate, disproportionate anger directed at the perceived source of rejection — a response that can look impulsive, volatile, or out of character given the client's baseline presentation.
The Neurobiological Roots of RSD in the ADHD Brain
Understanding why RSD happens — not just that it does — is one of the most clinically useful things a professional can offer a client. That shift — from "what's wrong with me" to "here's how my brain is wired" — changes the entire therapeutic conversation.
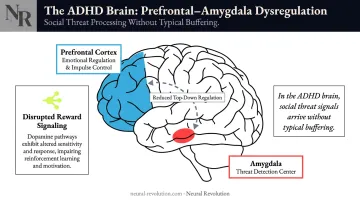
Prefrontal-Amygdala Dysregulation
ADHD involves structural and functional differences in two interacting systems: the prefrontal cortex (responsible for emotional regulation, impulse control, and executive function) and the amygdala (the brain's threat detection center). In the ADHD brain, these circuits communicate differently.
Research examining amygdala reactivity and prefrontal coupling in ADHD supports this picture — studies on amygdala reactivity and ventromedial prefrontal cortex coupling indicate that emotional stimuli, particularly social threat signals, are processed with less top-down regulatory control. They land at full intensity without the buffering that neurotypical emotional processing typically provides.
A separate line of research on lateral prefrontal cortex functioning during emotional interference in adults with persistent ADHD symptoms found associations with affect lability — confirming that emotional dysregulation is rooted in neurological structure, not personality.
The Dopamine Connection
ADHD involves disrupted dopamine neurotransmission across reward and motivation pathways. This matters for RSD because social approval operates as a reward signal. When that approval is withdrawn — or perceived to be — the relevant circuits register the loss faster, more intensely, and with more staying power than in neurotypical brains.
Why This Reframe Matters Clinically
RSD in ADHD is not caused by adverse childhood experiences, though trauma can intensify it. This distinction is critical for treatment planning.
Two implications follow from this:
- The primary clinical focus should be regulation and self-awareness building — not trauma processing
- Adverse experiences may be a concurrent issue requiring separate attention, but they are not the origin point of RSD in this population
How RSD Manifests in Clients: What Professionals Need to Recognize
An RSD episode has a recognizable signature: sudden emotional flooding that feels completely disproportionate to what triggered it, an inability to "logic out" of the feeling in the moment, and — critically — a relatively rapid return to baseline once the perceived rejection is resolved or reframed.
That last feature is diagnostically useful. It distinguishes RSD from sustained mood disorder episodes, which do not resolve this quickly. In practice, that distinction matters — because the behavioral patterns RSD produces are often misread entirely.
Behavioral Patterns in High-Achieving Adults
In professional contexts, RSD rarely presents as emotional volatility that's obvious to observers. It's more likely to show up as one of these patterns:
The people-pleaser. Clients who have spent years scanning social environments for approval cues and carefully curating how they're perceived. In high-achieving ADHD adults, this reads as professionalism, adaptability, or likability — until the cost to identity and autonomy becomes visible. Many clients arrive at coaching having managed others' perceptions for years without recognizing it as an RSD protective strategy.
Avoidance-driven perfectionism. Clients pursuing impossible standards not from genuine ambition, but as a preemptive shield against criticism. They may appear highly motivated while actually operating from chronic fear. You'll notice this as task paralysis, inability to submit work that isn't "perfect," or avoidance of new challenges where they might fall short.
The "stop trying" pattern. Clients who withdraw from opportunities, relationships, or leadership roles because the anticipated emotional cost of rejection exceeds the perceived reward. This is frequently misread as low motivation, imposter syndrome, or depression. More often, it's RSD doing what it does: making avoidance feel safer than risk.
Impact on the Professional Relationship
The coaching or therapeutic relationship itself can become an RSD trigger. Clients with RSD may experience feedback, adjusted goals, shifted session times, or even a coach taking a week off as rejection — particularly if the relationship feels evaluative.
Professionals should be intentional about:
- How feedback is framed — lead with genuine acknowledgment before critique, and be explicit about intent
- How missed sessions are handled — a neutral, matter-of-fact tone matters more than you might expect
- How sessions close — a forward-facing closing statement reduces the ambiguity that RSD feeds on
- Proactive check-ins after challenging conversations, rather than waiting to see if the client resurfaces
Differential Diagnosis: When RSD Looks Like Something Else
RSD is frequently misidentified — and the clinical consequences of that matter. Here's where the confusion most commonly occurs:
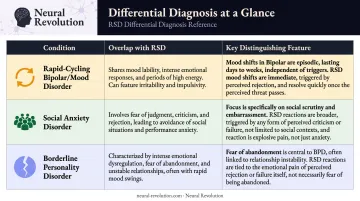
| Condition | Overlap with RSD | Key Distinguishing Feature |
|---|---|---|
| Rapid-cycling bipolar/mood disorder | Sudden shift from stable to devastated | RSD is triggered by a specific perceived rejection, not internal cycling; resolves quickly |
| Social anxiety disorder | Hypervigilance, anticipatory avoidance | RSD is episodic and tied to specific feedback; social anxiety is more diffuse and anticipatory |
| Borderline personality disorder | Emotional intensity, fear of rejection/abandonment | RSD does not include unstable self-image, chronic relationship instability, or dissociative symptoms |
The RSD–BPD Distinction
This is the most consequential misidentification in clinical practice. Both presentations involve emotional intensity and fear of rejection — but the differences are meaningful:
- RSD episodes are tied to a specific trigger and resolve relatively quickly
- BPD involves pervasive identity disturbance, ongoing relationship instability, recurrent self-harm or suicidality, and stress-related dissociation — none of which are characteristic of RSD in ADHD
- Misdiagnosing RSD as BPD leads to inappropriate treatment and can cause real harm
If a client presents with apparent mood instability that tracks specifically to interpersonal feedback or perceived social evaluation — and carries an ADHD diagnosis or shows ADHD symptoms — RSD should be actively considered. Not added as an afterthought.
RSD in AuDHD Presentations
For clients who carry both autism and ADHD diagnoses, the presentation can be more complex. Emotional flooding from RSD may layer with autistic shutdown patterns, sensory overload, or masking collapse — creating a picture that is harder to untangle and requires both lenses simultaneously.
The clinical priority here is to resist defaulting to a single explanatory framework when both neurotypes are present — neither diagnosis alone captures the full picture. Neural Revolution's coaching team includes practitioners with specific AuDHD expertise who work with this profile directly.
Practical Strategies for Professionals Supporting Clients with RSD
Start with Psychoeducation
Simply naming RSD for a client is often one of the most impactful things you can do. Many adults with ADHD have spent years — sometimes decades — interpreting their emotional intensity as evidence that they are "too much," broken, or fundamentally flawed.
Giving this experience a name, and grounding it in neurology rather than character, is a dignity-restoring clinical act. The framing matters: this is how their brain is wired, not a reflection of who they are.
One practical approach: surface RSD as a named friction point during intake, rather than waiting for it to emerge mid-engagement when it has already been activated and the relational dynamic is harder to navigate.
Clinical and Coaching Interventions
Medication (for clinical providers and prescriber collaborators)
Standard ADHD stimulants do not reliably address RSD. Per Dodson's clinical framework, alpha-agonists — guanfacine or clonidine — have shown the most consistent effectiveness for RSD specifically. For more refractory cases, MAOIs (particularly tranylcypromine) have been used off-label by experienced clinicians. Dosing decisions remain with prescribers.
Cognitive and Behavioral Strategies
CBT can help clients build self-awareness and identify patterns — but it has limited effect during acute RSD episodes, when the prefrontal cortex is effectively offline and reasoning is inaccessible.
The more useful clinical application is building pre-episode awareness: helping clients map their personal triggers, develop grounding protocols, and practice self-compassion scripts in calm states so those tools are accessible when activated.
The Distinct Role of ADHD Coaching
While clinical therapy targets symptom management, ADHD coaching addresses the functional and structural patterns RSD creates in daily life — a complementary focus, not a competing one.
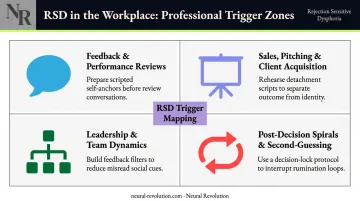
At Neural Revolution, the coaching approach — grounded in cognitive psychology and lived ADHD experience — works with high-achieving adults to identify what's driving RSD-fueled avoidance, perfectionism, and professional withdrawal. This includes trigger mapping in the specific contexts where RSD tends to be most disruptive:
- Feedback conversations and performance reviews
- Sales, pitching, and client acquisition situations
- Leadership dynamics and team relationships
- Post-decision spirals and second-guessing loops
Communication Principles for RSD-Prone Clients
Regardless of professional role, these principles reduce the risk of inadvertent RSD activation in your interactions:
- Lead with acknowledgment before critique — don't open with the problem
- Be explicit about intent: "I want to share something I think will help, not criticize you"
- Avoid ambiguous phrasing — vague feedback is a blank canvas for worst-case interpretation
- Close sessions with a forward-facing statement — something specific about next steps or the next contact point
- Check in proactively after a challenging session, rather than waiting to see if the client returns
Frequently Asked Questions
Do all people with ADHD experience rejection-sensitive dysphoria?
RSD is not universal, but it's extremely common — leading clinicians estimate the vast majority of adults with ADHD experience it to some degree, and a 2023 qualitative study confirmed RSD-like experiences in most participants. Presentation varies widely: some clients arrive with clear awareness of the pattern; others have never had language for what they've been living with.
What does a rejection-sensitive dysphoria (RSD) meltdown look like in people with ADHD?
The typical acute episode involves sudden emotional flooding — intense shame, rage, or despair — triggered by a perceived slight that may appear minor to an outside observer. The intensity is neurological, not theatrical. Once the perceived rejection is resolved or reframed, the person tends to recover relatively quickly, which distinguishes it from sustained mood episodes.
What is rejection-sensitive dysphoria (RSD) in ADHD and autism?
Both ADHD and autism involve heightened sensitivity to social feedback. In AuDHD individuals, this sensitivity can be amplified and more complex — emotional flooding from RSD may combine with autistic shutdown or sensory overload, creating layered presentations that require attention to both neurotypes simultaneously rather than collapsing everything into one diagnosis's framework.
How do you manage rejection-sensitive dysphoria in ADHD?
Management is multi-modal. Psychoeducation comes first — naming RSD often brings immediate relief. From there, trigger mapping and grounding strategies are built during calm states, not in crisis. For clinical cases, medication consultation is warranted (alpha-agonists are first-line per Dodson). ADHD coaching addresses the behavioral and relational patterns RSD creates over time.
Can RSD be mistaken for borderline personality disorder or bipolar disorder?
Yes — frequently. Rapid emotional shifts can mimic bipolar cycling, and fear of rejection overlaps with BPD presentation. The distinguishing features of RSD are that episodes are tied to a specific perceived rejection trigger, resolve relatively quickly, and occur within the broader context of an ADHD presentation rather than alongside chronic identity instability or dissociation.
What is the role of ADHD coaching in managing rejection-sensitive dysphoria?
ADHD coaching addresses the functional patterns RSD creates in daily life — avoidance, perfectionism, people-pleasing, conflict withdrawal — by helping clients build self-awareness, design feedback-friendly professional environments, and develop regulation strategies before the next episode hits. It complements clinical treatment when needed but operates in a distinct lane: performance and systems, not clinical symptom management.